 Virtual reality (VR) is an emerging technology that involves the interaction between a user and a computer with real time simulation of environments, functional activities, exercises and games. (Rutkowski et al., 2020). The definition of VR is based on the concept of “presence” which relates to the sense or feeling of being in an all-surrounding environment. There are currently 4 main types of VR:
The sense of ‘presence’ depends on the level of VR immersion. This is dependent upon the type of system used. In healthcare, VR is generally referred to as “specialized” VR (i.e. specifically developed therapeutic VR systems) or gaming VR (i.e. commercial VR-game consoles). Mechanisms The rationale for the use of VR is that enhanced stimulation provided by an artificially generated environment leads to activation of motor learning processes by influencing exteroception and enhancing the feed-forward mechanism of motor planning through goal directed activities. Repetition of efficient movement may then lead to motor re-learning which may transfer to functional activities. The thinking is that the VR environment has the potential to stimulate supervised and reinforcement learning, based on augmented visual, acoustic and sensitive feedback. Clinical applications To date VR has more commonly been used in neurologic rehabilitation (stroke mostly) where VR has resulted in greater improvements in upper limb function compared with conventional rehabilitation. (Rutkowski et al., 2020) It has also been reported in a small number of studies in the geriatric population (falls) and paediatric population (Developmental Coordination Disorder, Cerebral Palsy) where evidence of improvement compared with conventional treatment for lower limb function, gait and balance is not growing and still conflicting. A few studies have been published investigating its use for orthopaedic rehabilitation. (Gumaa & Rehan Youssef, 2019). To date, virtual reality has not shown any significant benefit compared with conventional rehabilitation for RA, knee OA, ankle instability and following ACL reconstruction and there is insufficient evidence to draw any conclusions in fibromyalgia, back pain and following knee arthroplasty.(Rutkowski et al., 2020) Given it’s application to improving movement planning and motor control, I wondered whether there were applications for the shoulder instability population, specifically for those with atraumatic instability, or post-immobilisation following traumatic instability or surgical stabilisation. In these patient groups, there may be inhibition of important stabiliser muscles at motor cortex level. I didn’t find any studies on shoulder instability, but I found one study in which VR had been used in rehabilitation for subacromial impingement syndrome (SAIS). Virtual Reality for Subacromial Impingement Syndrome Virtual reality using Nintendo Wii (boxing, bowling and tennis accompanied by an avatar) was compared with capsular stretching, pectoral stretching, scapula strengthening and bilateral shoulder elevation exercises (Pekyavas & Ergun, 2017) in 30 patients with SAIS. Pain intensity was significantly improved in both groups, however the VR group reported statistically significant improvements in night pain VAS, and pain with Neer, Scapula Assistance and Scapula retraction test compared with the control treatment group. There was also a case report of significant shoulder pain in a hemiplegic patient that was preventing rehabilitation. The pain improved with the concurrent application of VR during passive mobilisation and stretching enabling progression with rehabilitation suggesting VR may have central effects on pain mechanisms. (Funao et al., 2021) Doseage Doseage was variable across all studies:
Summary My motivation for looking into this was to find out whether VR training may be a useful adjunct to neuromuscular rehabilitation for people with motor control impairments around the shoulder (e.g shoulder instability, scapula dyskinesis, persistent shoulder girdle pain). What I have taken out of what I have found is:
Will I be buying a VR set for my shoulder patients? Not yet, but I’ll be watching the literature closely, and if anyone is looking for a research project, how about looking at the use of VR in the shoulder instability population? 😉 References Funao, H., Tsujikawa, M., Momosaki, R., & Shimaoka, M. (2021, Jul). Virtual reality applied to home-visit rehabilitation for hemiplegic shoulder pain in a stroke patient: a case report. J Rural Med, 16(3), 174-178. https://doi.org/10.2185/jrm.2021-003 Gumaa, M., & Rehan Youssef, A. (2019). Is Virtual Reality Effective in Orthopedic Rehabilitation? A Systematic Review and Meta-Analysis. Physical Therapy, 99(10), 1304-1325. https://doi.org/10.1093/ptj/pzz093 Pekyavas, N. O., & Ergun, N. (2017, May). Comparison of virtual reality exergaming and home exercise programs in patients with subacromial impingement syndrome and scapular dyskinesis: Short term effect. Acta Orthop Traumatol Turc, 51(3), 238-242. https://doi.org/10.1016/j.aott.2017.03.008 Rutkowski, S., Kiper, P., Cacciante, L., Cie?lik, B. a. e., Mazurek, J., Turolla, A., & Szczepa?ska-Gieracha, J. (2020, 11/19). Use of virtual reality-based training in different fields of rehabilitation: A systematic review and meta-analysis. Journal of Rehabilitation Medicine, 52(11), 1-16. https://doi.org/10.2340/16501977-2755
5 Comments
Musculoskeletal physiotherapists have a therapeutic ‘bag of tricks’ that includes a range of interventions such as advice, pain science education, acupuncture, exercise and manual therapy to name a few. What turns a ‘trick’ into an effective ‘treatment’ is its application within a biopsychosocial framework, guided by clinical reasoning, informed by evidence within a person-centered, shared decision-making model of care. Manual therapy as a “low-value” treatment Manual therapy has been the subject of mounting criticism for being a passive, low value intervention that has potentially nocebic effects, that can create dependency, foster maladaptive beliefs and create unrealistic expectations of treatment. This assumes that manual therapy is applied indiscriminately, in isolation, without clinical reasoning or context. If that is the case, I would be the first to agree that manual therapy, and any other treatment applied in this way, literally becomes another ‘trick’ of the trade. So what turns our manual therapy ‘tricks’ into an effective treatment for shoulder pain? Identifying “Responders” Like every other physical therapy intervention, manual therapy should be selected based on clinical reasoning throughout the assessment, diagnosis and treatment planning process to identify those people who are most likely to benefit from it. Deciding whether manual therapy may be an effective treatment tool starts during the assessment. In my experience, the ability to modify a persons’ symptoms during the movement-based assessment suggests the person may benefit from the inclusion of manual therapy as an adjunct to their treatment programme. Indeed, evidence has shown that the ability to change shoulder symptoms and/or range of motion of shoulder elevation with manual facilitation of the scapula was associated with better functional outcomes of treatment for shoulder pain. 1 There are many forms of manual therapy ‘symptom modification’ techniques described for shoulder girdle pain 2-4 These are applied during the provocative movement (usually flexion or abduction) to the shoulder and surrounding areas (e.g cervicothoracic spine) and change in pain is measured. An improvement in pain with a manual therapy technique suggests a mechanical/nociceptive (vs nociplastic or neuropathic) flavour to the pain phenotype. Based on our understanding of nociplastic and neuropathic pain mechanisms, it is unlikely either of these would exhibit an immediate reduction in pain with a manual therapy intervention. Mechanisms of symptom improvement While our early assumptions were grounded in the biomechanical model, we now know that combinations of neurophysiologic changes, endogenous pain control mechanisms, placebo and contextual effects can all interact to result in improvements in pain with manual therapy. While we may never be certain which of the myriad mechanisms is responsible for the improvement for any given person, an improvement suggests the person may ‘respond’ to manual therapy. Does the mechanism matter? No, but it matters how we explain the improvement to the patient to avoid maladaptive beliefs about the manual therapy “magic trick” that may create unrealistic expectations, lead to unnecessary health-seeking behaviour or foster dependency. Manual therapy as a treatment for shoulder pain The addition of manual therapy has been shown to improve treatment outcomes for pain and function for people with subacromial pain 5 and frozen shoulder.6 Scapula, humeral and cervicothoracic manual therapy techniques can be valuable adjuncts to treatment when they reduce pain and facilitate functional movement. Once functional movement is established, load can then be increased to build capacity within a multi-modal, movement and exercise-based programme. There are other ‘non-specific’ benefits too. The application of manual therapy creates space within the clinical encounter to hear the patients’ story and develop the therapeutic alliance. The enhanced level of trust this affords often leads to the disclosure of other, more personal information, that may also influence treatment outcomes. The ability to change symptoms gives the person hope that there may be a way to improve their symptoms, the level of trust in the practitioner increases and I find I get instant engagement with the treatment and exercise rehabilitation plan from that point on. The person is more confident to move, is less fearful that ‘something serious is wrong’ and when they can replicate this at home it gives them a self-management strategy for symptom improvement. Case examples: Here are two recent examples of patients I have seen who responded well to manual therapy:
Manual therapy can be an effective adjunct to treatment for people with shoulder pain when delivered within a multi-modal programme. When applied within a clinical reasoning model and aligned with the persons beliefs and realistic expectations it can be an effective treatment to help reduce symptoms and facilitate improvements in movement and function. Don’t treat manual therapy like a “trick” and you may start to see it as an effective treatment for the right person. References 1. Chester R, Jerosch-Herold C, Lewis J, Shepstone L. Psychological factors are associated with the outcome of physiotherapy for people with shoulder pain: A multicentre longitudinal cohort study. British Journal of Sports Medicine. 2016. 2. Lewis JS. Rotator cuff tendinopathy/subacromial impingement syndrome: is it time for a new method of assessment? British Journal of Sports Medicine. 2009;43(4):259-64. 3. Satpute K, Reid S, Mitchell T, Mackay G, Hall T. Efficacy of mobilization with movement (MWM) for shoulder conditions: a systematic review and meta-analysis. J Man Manip Ther. 2022;30(1):13-32. 4. Aytona MC, Dudley K. Rapid resolution of chronic shoulder pain classified as derangement using the McKenzie method: a case series. J Man Manip Ther. 2013;21(4):207-12. 5. Pieters L, Lewis J, Kuppens K, Jochems J, Bruijstens T, Joossens L, et al. An update of systematic reviews examining the effectiveness of conservative physical therapy interventions for subacromial shoulder pain. J Orthop Sports Phys Ther. 2020;50(3):131-41. 6. Noten S, Meeus M, Stassijns G, Van Glabbeek F, Verborgt O, Struyf F. Efficacy of Different Types of Mobilization Techniques in Patients With Primary Adhesive Capsulitis of the Shoulder: A Systematic Review. Archives of Physical Medicine and Rehabilitation. 2016;97(5):815-25.  Dr Angela Cadogan, PhD, NZRPS Frozen shoulder is still poorly understood on many levels. However the diagnostic criteria for have remained unchallenged for decades: Frozen shoulder is a clinical diagnosis characterised by:
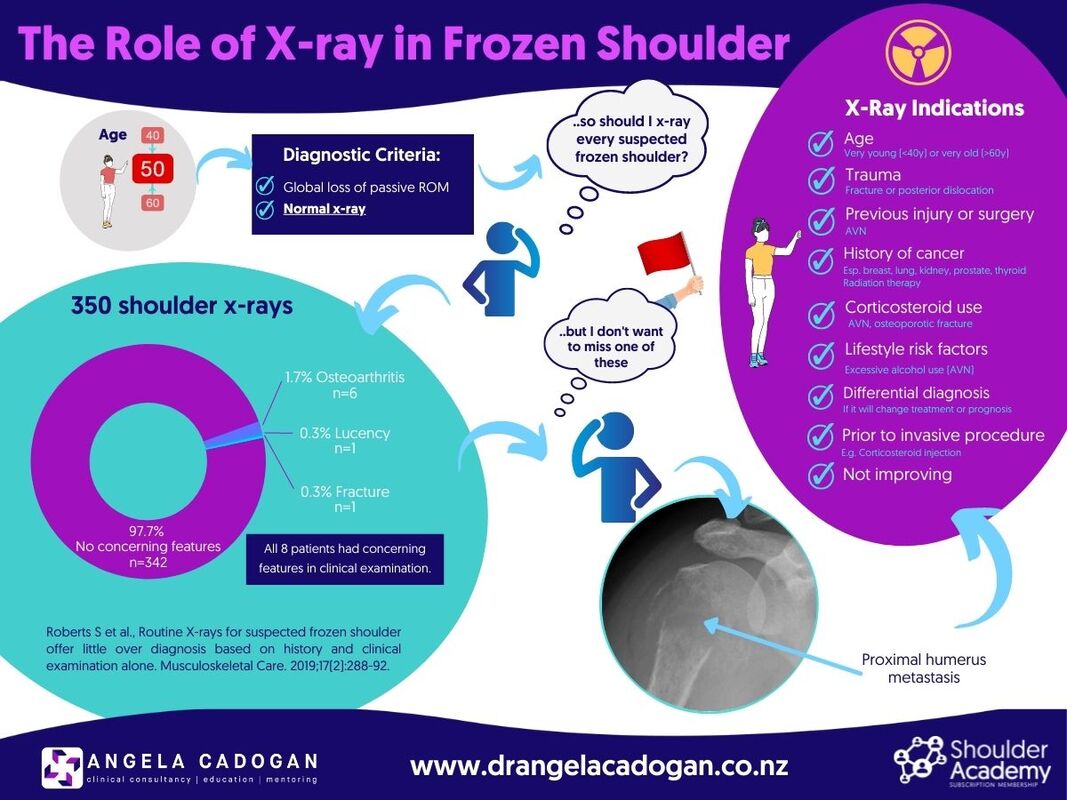
In my career, I have seen people diagnosed and treated for frozen shoulder for more than 2-3 years with a ‘wait and see’ approach, or with multiple injections without an x-ray to exclude other causes of stiffness. Some of these people were subsequently diagnosed with osteoarthritis, avascular necrosis, and (one) posterior dislocation. Other causes of shoulder pain and stiffness include primary or secondary bone tumour, traumatic, osteoporotic or pathologic fracture and muscle guarding. However evidence from the UK reported the percentage of those with suspected frozen shoulder who had abnormalities on x-ray to be low (2.3%), and those who had abnormalities all had ‘concerning’ features in their clinical examination. The argument is that ‘routine x-rays for suspected frozen shoulder offer little over diagnosis based on history and clinical examination alone’, and that not all frozen shoulders need an x-ray. Regardless of the yield rate of serious pathology, a normal x-ray is part of the diagnostic criteria for frozen shoulder. Whether or not you choose to request one is an entirely different matter. If there is no x-ray, you cannot exclude other causes of stiffness. Excluding other conditions becomes more important when there are 'concerning' features in the history, and as the patient moves through the health system into secondary and tertiary care. Referral to specialist services usually means they are not responding as expected and differential diagnosis becomes increasingly important. Your decision as to whether an x-ray is needed therefore comes down to probability-based clinical judgement and how much clinical risk you are prepared to accept, combined with documented informed consent processes so the patient understands the potential risks of not obtaining an x-ray if frozen shoulder is suspected. In New Zealand, x-ray imaging is readily available, accessible, affordable for most and are required before a corticosteroid injection can be administered (under imaging guidance) to the glenohumeral joint as part of guideline-based treatment for pain. However, there may be some countries, regions and healthcare settings where x-rays are not readily available due to lack of access, funding or radiology resources, lack of practitioner referral rights, or x-ray may be contraindicated in some cases (e.g pregnancy). In this case priority for x-ray would go to those with red flags or risk factors for potentially serious pathology from the clinical examination such as those listed above or where it will alter treatment or prognosis (e.g osteoarthritis). In the infographic below I've tried to provide a list of factors which would prioritise x-ray imaging for people with suspected frozen shoulder. Key Message: The key message here is: don’t confuse diagnostic criteria with probability-based clinical decision-making. No x-ray = no ability to exclude other causes of stiffness, regardless how rare or common abnormalities may be. Choosing not to request x-ray is a decision for the individual clinician in their unique setting based on risk assessment, patient informed consent and availability of imaging resources. More shoulder learning resources: Frozen Shoulder: https://bit.ly/3q92Ani What’s New In Physiotherapy Management of Frozen Shoulder: https://bit.ly/3hFCsPn Reference: Roberts S, Dearne R, Keen S, Littlewood C, Taylor S, Deacon P. Routine X-rays for suspected frozen shoulder offer little over diagnosis based on history and clinical examination alone. Musculoskeletal Care. 2019;17(2):288-92.
 A few weeks ago I wrote a post about the level of clinical competency required at specialist levels of physiotherapy practice which generated a bit of interest. I mentioned that my experience of working at this level (compared with other levels of practice) is the expectation that the specialist physiotherapist will have a solution we are others have failed. Often we are ‘expected to know’. In the previous post I discussed some of the factors that contribute to ‘complexity’. So how do I approach and interpret my assessment and make decisions about appropriate treatment given that many people I see have already had many investigations and treatment, often from very competent professionals? In my practice, people tend to fall into one of two groups:
With these two groups in mind, I’ve put together some of the common processes I have found helpful for guiding my decision-making when seeing specialist patients.
I’d love to hear whether other Specialist Physiotherapists have any other tips, or whether this helps other physiotherapists out there to organise your thinking and develop a framework for troubleshooting challenging clinical presentations. If you’re interested in hearing more about how to reason through challenging clinical situations you may be interested in this recorded webinar hosted by Physio Academy. Problem Solving the Problem Shoulder: 3 Reasons They’re Not Improving 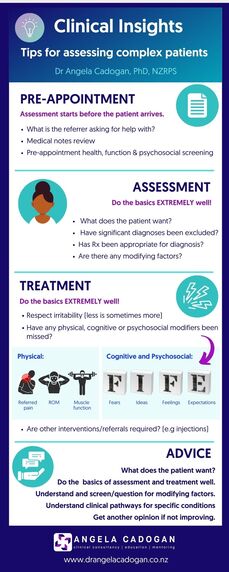 |
Dr Angela CadoganPassionate about learning and helping others to think critically about their practice. I hope these posts stimulate your thinking and help you in clinical practice. Archives
November 2022
Categories
All
|
||
 RSS Feed
RSS Feed
